Open Access Journal of Dental and Oral Surgery
[ ISSN : 2833-0994 ]
The Treatment of the Anterior Crossbit using an Eruption Guide Appliance with Different Thicknesses: Case Report
Studio odontoiatrico Pellegrino, Via G A Acquaviva, 37 Caserta, Italy
Corresponding Authors
Keywords

Abstract
An anterior crossbite can be functional, when there is a precontact that generates a mandibular protrusion, or skeletal, a characteristic and early sign of a Class III. An anterior crossbite, both functional and skeletal, if not treated, can lead to a sharp worsening of the malocclusion, causing psychosocial and functional inconveniences. The use of eruption guide appliances (EGA) with different thicknesses can approach this problem very effectively and quickly. In addition, the usability of the device allows to get an excellent collaboration from the patient.
Introduction
Anterior crossbite is an anomaly in the anterior-posterior plane. This anomaly is very popular in the III classes. The anterior cross bite can be generated by many factors: functional, skeletal or dental [1]. When it is of dentoalveolar type, it can be caused by dental lingual eruption, delayed eruption of the upper incisors, labial inclination of the lower incisors, or the presence of supernumerary teeth; in addition, it can be caused by resting lingual malposition, mandibular malposition habit or oral respiration. The skeletal type anterior crossbite is characterized by an alteration of the size or position of the maxillary and mandible. The skeletal component presents with a mandibular prognathism, maxillary retrognatism or a combination of both. Maxillary deficits on both the sagittal and vertical plane may cause a Class III malocclusion. The cause can be direct if the maxillary is positioned posteriorly or is underdeveloped; or indirect when it has a deficit in vertical growth. Lower vertical growth of the maxillary involves a counterclockwise rotation of the mandible, producing a mandibular prognathism effect. As has been widely reported in numerous studies, the hereditary factor and therefore genetics factors have a fundamental role in the origin and development of this malocclusion [2]. Asians are the population where this malocclusion is most evident [3].
In functional anterior crossbite or pseudo class III, the mandible in closure is positioned anterior to the upper jaw. Usually this is due to premature dental contacts [4]. This type of crossbite is the most common. For the functional crossbite diagnosis, it is important to assess whether a dental precontact or interference causes a functional shift between centric relation (RC) and centric occlusion (OC). In the anterior crossbite, the dentoalveolar component presents with an upper incisors proclination and a lower incisors retroinclination [5-6]. The dentoalveolar component represents an important interface because it is the one that responds most to stimulation by orthodontic appliances. It is extremely important to treat anterior crossbite in primary or mixed dentition by eliminating the causes early, to restore proper growth and development. If allowed to progress, it encourages the worsening of malocclusion of class III, causing both psychosocial and functional difficulties to the patient. Treating and resolving anterior crossbite in childhood significantly reduces the severity of the malocclusion development but also improves the patient’s life [7]. There are different ways to treat anterior crossbite and third classes in deciduous and mixed dentition. The most frequent and the best known is based on a sagittal approach such as the facial mask, to which is added a transversal component by means of a palatal disjunctor [8]. This type of approach is very effective in patients with a maxillary retrusion.
There are other ways of treatment in the literature such as: the use of SEC III [9] that adopts two acrylic splints with different thicknesses and elastic third class, or a variant like the PS3 that uses two acrylic splints and a Forsus ™ L-pin module for side, both accompanied by the use of chin cup [10]. The functional device Frankel III is also used for the interceptive treatment of malocclusion thanks to the labial shields that promote the forward growth of the upper jaw [11]. The objective of this case report is to demonstrate the effectiveness of the use of eruption guide appliance (EGA) for the interceptive treatment of the anterior crossbite and avoid the worsening of III classes. This approach differs from the classic methods that focus on sagittality, as it aims to treat malocclusion through greater control of verticality.
Materials and Method
Case Report
The patient is 7 years and 7 months old with a good state of health, absence of spoiled habits, joint disorders. He hasn’t done any orthodontic treatment before.
Extraoral analysis: For the sagittal analysis, the adopted parameter is the angle of the facial convexity. From the angle analysis, the facial profile appears to be convex. Whereas, from the analysis of the facial thirds, the patient presents the inferior third increased, traced from the subnasal point to the menton. The lower third rise is caused by the increased size of the mental labium portion. While the nasolabial corner is open. This indicates a lingual inclination of the upper incisors, resulting in a flat lip profile. For the extraoral vertical analysis, the steepness of the mandibular plane that indicates a dolicofacial (high angle) tendency is valutated.
Intraoral analysis: The patient has an early deciduous mixed dentition. Sagittally, the patient presents a deciduous mesial step and a III canine class on both sides, with an anterior crossbite. It is due to the presence of a precontact that caused the birth and the subsequent worsening of it, triggering a mandibular deviation. In particular, this functional cause occurs in the lower median that is deflected to the patient’s left relative to the upper interincisive line and the median line of the face (Figure 1 & 2).
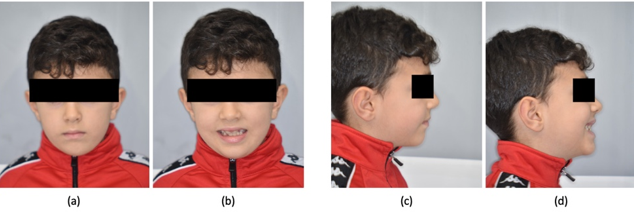
Figure 1: Extraoral pre-treatment pictures: (a) frontal view at rest; (b) frontal view with a smile; (c) lateral view at rest; (d) lateral vie with a smile.
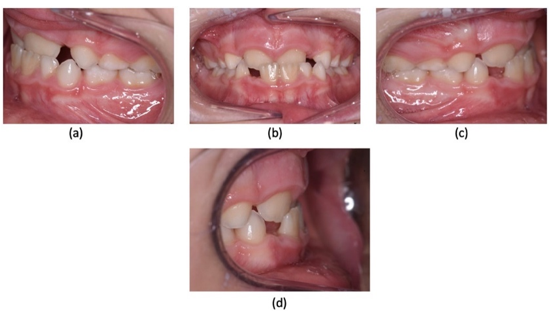
Figure 2: Intraoral pre-treatment pictures: (a) lateral view at left side; (b) frontal view; (c) lateral view at right side; (d) overjet.
Radiographic and hard tissue analysis
i. For the evaluation of hard tissues, two x-rays were taken, one latero lateral telecranium and one orthopantomography.
ii. From orthopantomography, the patient has early mixed deciduous teeth with all permanent teeth.
iii. From the telecranium a cephalometric analysis was performed.
iv. The patient has a skeletal I class (ANB: 3.6°), with a slight protusion of the upper maxillary (SNA: 83°).
v. The SN-GoGn angle value of 31° denotes a normodivergent growth pattern with a tendency to hyperdivergence due to a reduced mandibular ramus height, measuring only 41.8 mm.
vi. The tendency to hyperdivergence is also evident from the FMA values that have been increased (FMA: 29°).
vii. the inclination of the occlusal plane is normal with values of 17°.
viii. The interincisive angle is increased (+1 -1: 144°).
ix. The lower incisors are retroclinated with an IMPA angle of 87° (Figure 3) (Table 1).
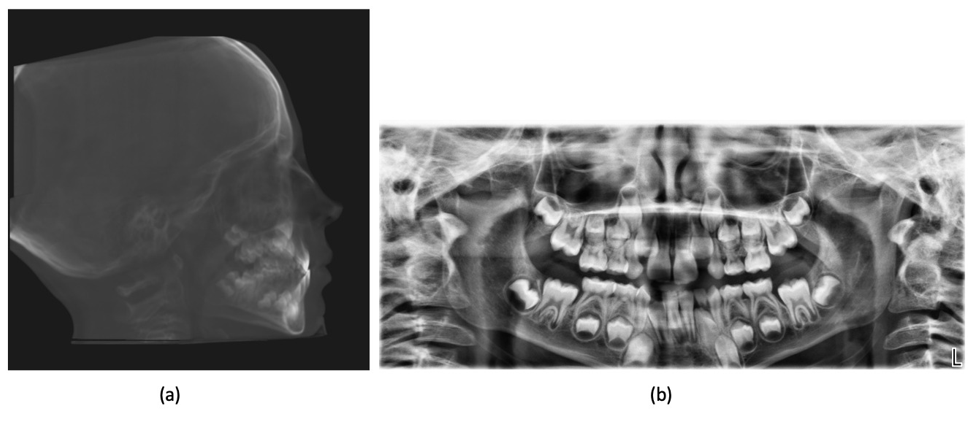 Figure 3: Pre-treatment radiographic records: (a) lateral cephalogram; (b) orthopantomogram.
Figure 3: Pre-treatment radiographic records: (a) lateral cephalogram; (b) orthopantomogram.
Table 1: Cephalometric data pre-treatment.
|
Parameters |
Normal range |
Recorded values |
|
SNA |
82° ± 2° |
83.34° |
|
SNB |
80° ± 2° |
79.71° |
|
ANB |
2° ± 2° |
-363° |
|
Wits |
-1 ± 2 mm |
-2.43 mm |
|
Occlusal plane to SN |
14° ± 4° |
17.76° |
|
SN-GoGn |
32° ± 2° |
31.67° |
|
Ramus height |
54.2 mm |
41.80 mm |
|
FMA |
25° ± 2° |
29.17° |
|
IMPA |
90° ± 2° |
87.44° |
|
Interincisal angle |
130° ± 5° |
144.47° |
|
Overjet |
2 ± 2 mm |
-0.36 mm |
|
Overbite |
2 ± 2 mm |
2.15 mm
|
Treatment
i. The device used is LM-Activator (LM-Instruments Oy, Parainen, Finland). The goal of treatment is to correct anterior crossbite to prevent the progression of malocclusion.
ii. The use of this device is linked to the diagnosis of Class I relationship.
iii. The use of the device was exclusively nocturnal, and was not changed or modified during treatment. The patient was asked to use it from after dinner until the following morning, so that the device could be used from 8 p.m. to 2 a.m., the time when there is a greater release of the somatotropic hormone GH.
iv. Orthodontic treatment is still ongoing but the goal has been achieved in just 5 months.
v. With resolution of the anterior cross bite, the patient will continue to use the device to maintain ideal growth control and improved dental occlusion due to the presence of the slots. From future follow-ups, we expect an improvement in mandibular ramus length resulting in mandibular anterotation. This will cause further improvement in the patient’s profile.
Results
In the fourth month after the start of treatment, the patient has a double occlusion, one in head to head and another in anterior crossbite, representing how the patient continued to cooperate. The occlusion in the head to head manifests itself in the minutes following the removal of the device and then returns in anterior crossbite. This indicates a collaboration of the patient. The exposure of the smile also changes and, above all, we can see from the extraoral profile photos an increase of the lower third and a more convex profile. This is caused by the increase of the overbite. This apparent facial profile elongation is a transient phase due to the presence of precontacts induced to the functioning of the device (Figure 4-6).
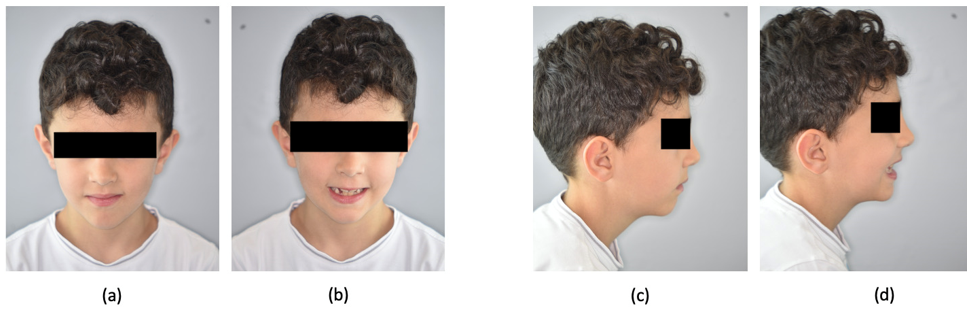
Figure 4: Extraoral pictures after 4 months of treatment: (a) frontal view at rest; (b) frontal view with a smile; (c) lateral view at rest; (d) lateral view with a smile.
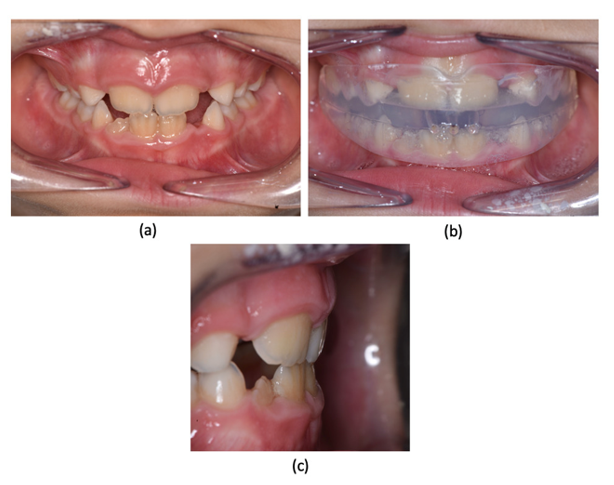
Figure 5: Intraoral pictures after 4 months of treatment: (a) frontal view; (b) frontal view with EGA; (c) overjet
After 5 months from the start of treatment, the patient resolves the anterior cross bite, having only one occlusion with a positive overjet and a positive, but still increased, overbite.
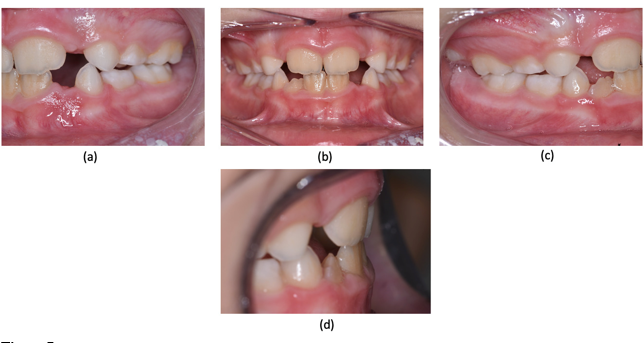
Figure 6: Intraoral pictures after 5 months of treatment: (a) lateral vie wat left side; (b) frontal view; (c) lateral view at right side; (d) overjet.
The treatment is not finished yet because we want to further improve the overjet and overbite. After a year in agreement with the guiding principle of As Low As Reasonably Achievable (ALARA) we will proceed to the realization of new radiographs to analyze further changes in the skeletal plane, in order to evaluate the improvement of both the inclination of the occlusal plane and of the length of the mandibular ramus.
Discussion
The device used in this case report controls the vertical dimension through the presence of different thicknesses that allow to control the dental eruption. In this case the device has a greater thickness in the posterior area, and a smaller thickness in the anterior area. This morphology consents a stimulation of the growth of the mandibular ramus, thus favoring a mandibular anterotation [12] using the contemporary vertical control of masticatory muscles. This type of approach is similar to other orthodontic devices like bite block and interarches splints (Splint Elastics Chin cup III), where on the front, the resin plate has a lower thickness in order to favor an anticlockwise rotation of the mandible, helped also by the use of the chin cup. The effect given of the III class elastic bands present in SECIII within the EGA is achieved by the musculature which generates a similar effect by closing the lips [9].These types of changes in verticality were reported in the Keski-Nisula study, which investigated how the use of EGA can actually cause tooth-to-face changes, especially in the vertical plane with an increase of mandibular ramus length by an improvement in the condylar growth [13]. This allows to control the inclination of the occlusal plane that in agreement with Tanaka and Sato represents the most important component that affects the third facial middle [14].
Changes in the occlusal plane do not stop at the end of the growth peak but continue even during and after puberty with, what Proffit calls, the post-eruptive juvenile equilibrium. The analyses and the various case reports presented by Sato justify an important consideration, that in the third classes genetics is not the only one to have a fundamental role, but it is above all the inclination of the occlusal plane and therefore the molar eruption [15].The device used in this case report has two main features, the first is the presence of slots that allow the teeth to reach an ideal Class I occlusion and therefore to solve cases of dental crowding in advance. As mentioned above, the second and most important is the presence of different thicknesses. In this case the device has a greater thickness in the molar area and a smaller thickness in the front area. This feature allows to facilitate the resolution of the dental crossbite, thanks to the opening of the bite; but above all it allows to control the molar growth avoiding overeruption. The presence of the posterior thicknesses gives propioceptive stimuli at the periodontal level, controlling the molar eruption, but also at the level of the temporomandibular articulation and the condyle. The opening of the bite causes a distraction of the condyle that generates a response of the neighboring cells that allow a change in bone growth in that area. The dental eruption control allows to modify the mandibular plane inclination and in accordance with Moss’ studies of 1999 to restore the ideal inclination for a given patient depending to the growth pattern. Only a few studies have been carried out on the early treatment of anterior crossbite with a myofunctional approach using EGA [16-17]. In these studies, it stands out the enormous effectiveness of this approach, the enormous speed of resolution of the case, and especially the ease of application of the device compared to more bulky devices used for the same treatment.
Limits
The main limitation of this study is the absence of an X-ray assessment. In addition, the absence of studies with a long follow-up. The only ones are with a followup of 1 year and the results obtained from the treatment are not relapsed [18].
Conclusion
The efficacy of the approach to the treatment of functional anterior crossbite seems to be confirmed by increasing clinical data. A particularly significant advantage consists in the fact that this therapy is carried out with an exclusively nightly use of the device. In this way is possible to effectively treat an anterior crossbite that, if untreated, could compromise the patient’s quality of life both on the psychosocial aesthetic and on the functional level. Future research will be directed towards cephalometric analysis to evaluate any changes in the length of the mandibular ramus and consequently of the inclination of the occlusal and mandibular plane.
References
1. Proffit W, Henry F, Larson B, Sarver D (2018) Contemporary Orthodontics. 6th. Philadelphia, Mosby, USA, pp. 437-725
11. Fränkel R, Fränkel C (1989) Orofacial Orthopedics with the Function Regulator, Karger.